|
Narcolepsy
Mechanism
This section is technical and boring.
Scroll down the next if you can't take it.
There are many things, infectious or genetic or
otherwise which could cause orexin cell dysfunction. For numerous
theoretical reasons, and with many direct reports of remission, I am
convinced that gluten induced immune activity is responsible for most
cases of human narcolepsy.
The assumption that narcolepsy is an immune
disorder is easy:
Narcolepsy is associated with
the gene HLA DQB1-0602. Very Strongly Correlated. 90% of
patients with narcolepsy/cataplexy carry the gene.
The HLA area of the genome codes
for immune system molecules. That gene specifies a portion of an
antibody.
If you have a messed up antibody-
you have an immune disorder. That's just a fact.
-
In this
study, a stable structure for the
DQB1*0602 antigen bound to an orexin molecule was
determined. This would permit the antigliadin antibody to attach to
the structure and initiate destruction of the neurotransmitter
itself. It is unknown however, if this process actually occurs in
vivo.
Although this direct mechanism is appealing,
I
propose a less direct method of neural dysfunction caused by the
*0602 antibodies.
-
Many of the genes in the
HLA-DQB1 region are
highly associated with gluten intolerance- an allergy
to wheat. The locus is actually named CELIAC1.
-
The DQB1-0602 gene is specifically associated with NON-celiac gluten intolerance-
documented symptoms are endocrine and neurological dysfunction.
I believe that is becaues these antibodies bind to neurons rather
than epithelium.
The antigliadin study
shows that IgG antigliadin molecules bind to the protein Synapsin I.
Synapsin 1 is crucial
to neurotransmitter transport and release in neurons. If you
don't have functioning synapsin, your nerves can't release their
chemicals.
-
Synapsin is found
in the synaptic cleft, at the nerve terminal. It is
possible that the gluten antibodies bind to free synapsin, thereby
making it unavailable for reuptake and use by the cell.
-
There are also
processes which allow antibodies inside the cell, which would allow
them to bind to Synapsin 1 in situ and block neurotransmitter
release directly.
A number of factors contribute to the
presentation of narcolepsy.
It seems different combinations of
antibodies cause variation in the symptoms.
-
Narcoleptics are more likely to have
two copies of DQB1*0602. Certain other
combinations of HLA genes also
predispose to narcolepsy.
-
DQB1*0602 association was highest in
cases with orexin deficiency, most of
which had narcolepsy-cataplexy. A weaker DQB1*0602
association was present in cases without cataplexy.
-
DQB1-0603 and 0604
are slightly different but also associated with narcolepsy.
Which is also supported by
a very detailed
study on the structures of
antigen alleles in the DQB1 locus. It shows that minor differences in
the coding sequences of the alleles produces differences in the
antigen's ability to bind to target proteins. Minor alterations in
the amino acid sequence can create significant changes in the shape of
binding pockets on the antigen.
This parallels the
activity of the gluten antibodies.
___________________________________________________
Shorter Mechanism:
All the
evidence points to diet as the most probable cause of narcolepsy.
•
Orexin neurons innervate the entire
gastrointestinal tract and regulate
metabolism.
•
Inflammatory diseases of the gastrointestinal tract
have been shown to affect the function of orexin cells.
•
Autoimmune antibodies
have been shown to affect the function of orexin cells.
Here's what happens- after you eat gluten,
your immune system sends out the antibodies. They bind to
the gluten in your intestine, but also to the nerve endings in your
orexin cells, clogging them up. You get sleepy and take a
nap.
Heh. If only it were that simple...
Metabolic obstruction
by antigliadin explains the excessive sleepiness and orexin cell loss in
narcolepsy but does not account for some of the signature symptoms. Cataplexy is the sudden loss of muscle tone and
onset of REM sleep which is triggered by stress. The mechanism described
above suggests a delayed, more gradual onset of sleep associated with
meals. I propose that cataplexy is a separate mechanism of orexin
depletion caused by a spike in blood sugar in response to stress.
___________________________________________________
Glucose Sensing
Orexin cells aren't
ordinary.
All cells are
sensitive to their own internal glucose levels and moderate their
activity.
Unlike most brain
cells, orexin neurons are sensitive to external glucose levels.
By altering the amount of orexin released- they moderate the metabolic
levels of cells other than themselves in response to serum glucose
levels.
-
As blood sugar
rises orexin cells lower their activity.
-
As blood sugar
lowers they increase production of orexin.
-
There are
four
basic types of glucose sensors, each which senses a specific range
of concentration, facilitating the very rapid and very precise
sensing of changes in blood sugars.
-
This mechanism is
sufficiently sensitive to encode variations in glucose levels
reflecting those occurring between normal meals.
So every time you
eat you alter your orexin system and everything it regulates.
Even if you don't have gluten antibodies killing the cells.
You can shut them down just by spiking your blood sugar.
That story the "experts" tell you about the Thanksgiving turkey making
you sleepy- they're wrong. It's everything else- the
glorious pile of carbohydrates: potatoes, corn, stuffing, yams,
cranberries and pie...
Sleep Attacks
Narcoleptic
naps are just like real naps only more so. The sugar and gluten
gang up on your neurons and your orexin levels drop faster and go
lower...
Figure 1. Nap Map
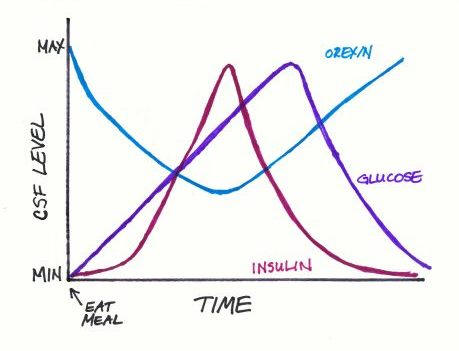
This is how I think a
narcoleptic sleep attack progresses:
Your blood sugar level
is low, and your orexin level is high so you're motivated to eat. If
you're American, then it's pretty well assured that your meal includes
carbs and gluten.
Your immune system
starts to produce antibodies.
As the food is
digested, your blood sugar starts to rise, so your orexin cells slow
down.
Soon after that the
gluten antibodies start clogging up the orexin cells.
At a certain point the
orexin levels fall below threshold and you fall asleep.
Lowering of orexin
levels stimulates the pancreas to release insulin.
Your orexin levels get
really low, and your pancreas doesn't know part of it is caused by
gluten instead of sugar, so dumps huge amounts of insulin into your
bloodstream.
Blood sugars drop
rapidly, and orexin levels begin to rise again.
And you wake up
wanting more sugar. So you go eat a cookie.
(If you look at it
carefully, it may be that part of the time we are sleeping because our
orexin levels are low, other times because our blood sugar is low.
Our levels fluctuate wildly after a meal.)
Cataplexy
Stress Response
Cataplexy is highly
associated with stress and panic. I believe the rapid rise in blood
sugar triggered by the stress response is the factor which triggers such
drastic symptoms.
Stress increases your
serum glucose levels. Rapidly.
Which shuts down your
orexin cells. Rapidly.
Which shuts off your
Locus Coerulus. Rapidly.
Glucose sensitivity
I believe that
one of the causes of cataplexy is atypical glucose sensitivity in orexin cells. I
considered a number of alternatives as to how that could occur. Perhaps
narcoleptics have extra sensitive mutant glucose sensors. Or an extra
gene and therefore produce more of them. But then I realized the
differential sensitivity of the cells would influence the pattern of
neurodegeneration and spontaneously result in increased glucose
sensitivity.
-
In addition to the
four ranges of glucose sensing,
orexin cells have two reactions to
rising glucose. 30% of them shut down and stay inactive until glucose
levels fall again. However, in the remaining 70% of orexin cells
activity first falls but then, despite high glucose levels, they
spontaneously resume firing.
Think about it: if
antigliadin binds to synapsin in cells when they are actively
transporting neurotransmitters, then those cells which shut down the
fastest and stay off the longest in response to glucose will have the
least damage from gluten. All the low and medium sensitive cells will clog up and
die. Sooner or later the hypersensitive orexin neurons will be the only
ones left.
If you have
accumulated a lot of cell damage- not only will you have fewer cells to
produce orexin, the ones you have will be, for practical puposes,
binary. Even small amounts of glucose will turn them all off.
______________________________
If the patient's blood
sugar is already raised, and he has an extra-sensitive set of orexin
cells, and his liver starts dumping glycogen, it may be just the right
combination for sudden onset of sleep. Each additional source of
glucose adds to the effect.
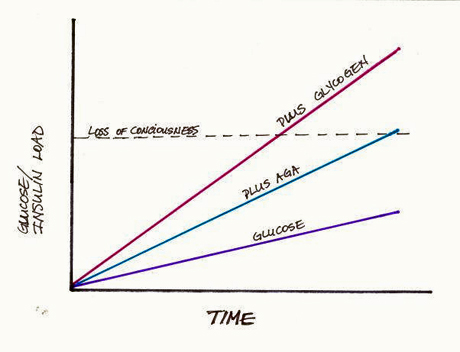
Figure 2. Additive
effects on orexin cells.
So here's the wicked
twist: Narcolepsy increases the stress response. Low orexin in the locus
coeruleus not only lowers your energy level but signals the vagus nerve
to
cause an increased startle response.
I believe this may cause
a positive feedback loop- vagus nerve activity stimulates activity of
the orexin cells which accelerates their uptake of the antibodies
causing even quicker shutdown of the cells.
It’s also possible the rapid
decrease in orexin triggers the stress response even further dumping
even more glycogen.
Or something like
that.
______________________________________
And on a slight
tangent- cataplexy often occurs during laughter.
-
Our human imaging
data also show that cataplexy patients have elevated responses to
humour in the left nucleus accumbens, a region known to be involved in humour processing
and which has strong interconnections with the amygdala.
These results
suggest that orexin physiologically modulates the processing of
emotional inputs within the amygdala, and the mechanisms of
cataplexy involve a dysfunction of hypothalamic-amygdala
interactions
I believe these
results make more sense if you consider
laughter as a modified version
of the panic response instead of as an indication of happiness. The
amygdala is one of the central processors of fear.
______________________________
This is also why alarm
clocks don’t wake you up: they induce narcolepsy as they startle you
awake. Induce a nice surge of glycogen from your liver.
You aren’t even
conscious and you’re having a sleep attack.
Good Morning!
____________________________
Orexin Expression
This graph represents
the orexin levels of a narcoleptic over a lifetime predicted by this
model:
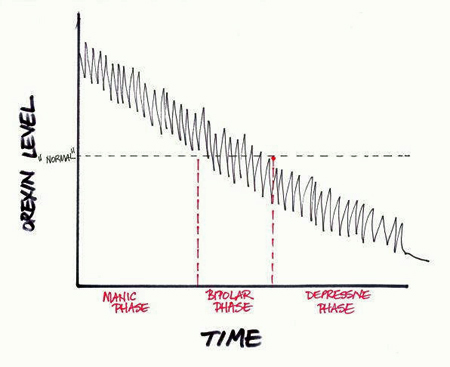
Figure 3. The sharp
learning curve
-
Highly active
orexin cells overproduce the neurotransmitter early in life.
-
Vigorous antibody
activity creates wildly fluctuating levels during daily activity.
-
Cumulative
neurodegeneration results in ever diminishing numbers of cells and
overall orexin levels.
-
At a certain point
levels begin to drop to the point affective symptoms become
apparent, but are intermittent.
-
Eventually orexin
levels drop to the point that daily functioning is chronically and
severely impaired.
If you want to be
specific, that was a narcoleptic male. Orexin levels in females also
fluctuate with reproductive hormones, so it adds another level of
variance.
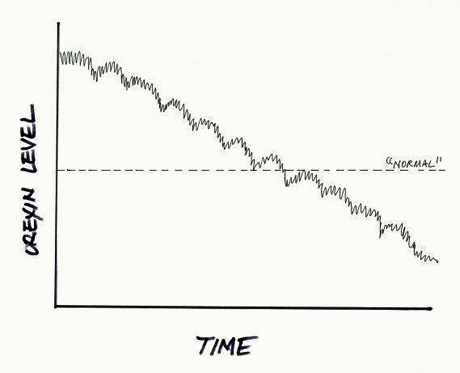
Figure 4. The emotional roller-coaster
Look at that-
it predicts that some of you haven't killed all your cells yet...
__________________________________________
So- I hope I have at
least made this much clear- there are a number of overlapping
factors that contribute to the symptoms of narcolepsy. The
combination you have determines your combination of symptoms.
-
Gluten antibody
response- which combination of antibodies you produce and how much
-
Cumulative damage-
how many orexin cells you have lost.
-
Primary insulin
response -occurs before you eat. If you wait too long and allow your
blood sugar get too low you will have dizziness and other symptoms
before you eat.
Secondary insulin response-occurs after you eat.
We produce too much and the result is hypoglycemia. Women seem
more susceptible to this than men.
-
Stress response.
This varies with age and infection status. And men seem
to have stronger responses than women.
-
Your diet.
Since orexin cells sense glucose, what you eat has the biggest
effect of all.
And these factors
change as the pathology accumulates.
For example, there's
this interesting metabolic alteration that happens-
Glucose sensitivity
amplifies over time. But insulin
response wanes as you age.
If you're lucky, they
kind of cancel eachother out.
There are also a
couple things that mimic cataplexy- and we are susceptible to both
of them.
Those topics are
covered later.
_____________________________
Recommended Reading:
New Mechanism Explains
Glucose Effect On Wakefulness
Why Sugar Makes Us Sleepy (And Protein Wakes Us Up)
Illness affects Orexin Cells
Special thanks to
JL for insisting that glucose was involved and forcing me to reassess my
paradigm. I was totally missing the big picture. He was so sure, he
underwent a glucose tolerance
test with real-time insulin monitoring.
After ingesting the glucose, he had a complete cataplectic attack, and
while he was out- his insulin jumped THREE TIMES normal levels. That’s
alarming.
(And his doctor
told him he was imagining it too.)
|